SafeBVM’s flagship innovation, the award-winning Sotair® device, is primarily funded by grants and contracts from the National Institutes of Health (NIH), the National Science Foundation (NSF), and the U.S. Military.
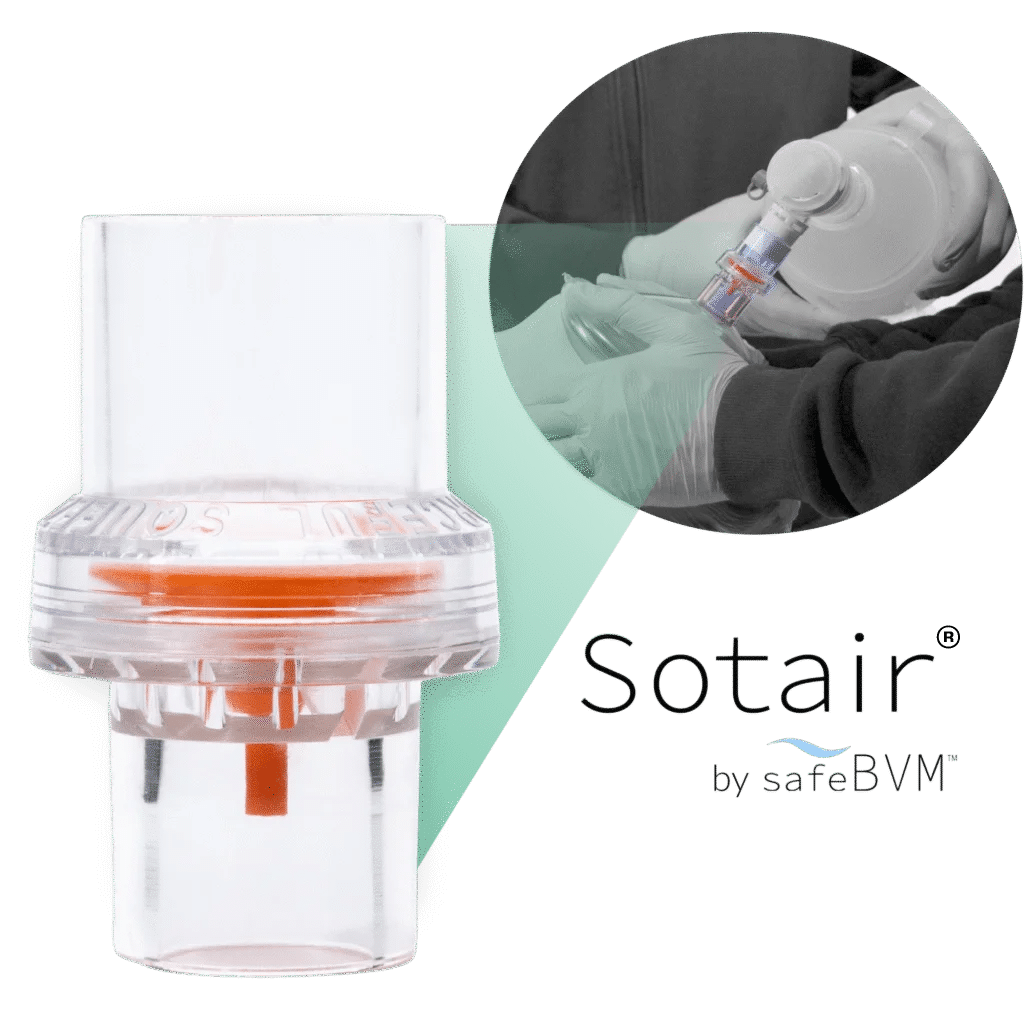
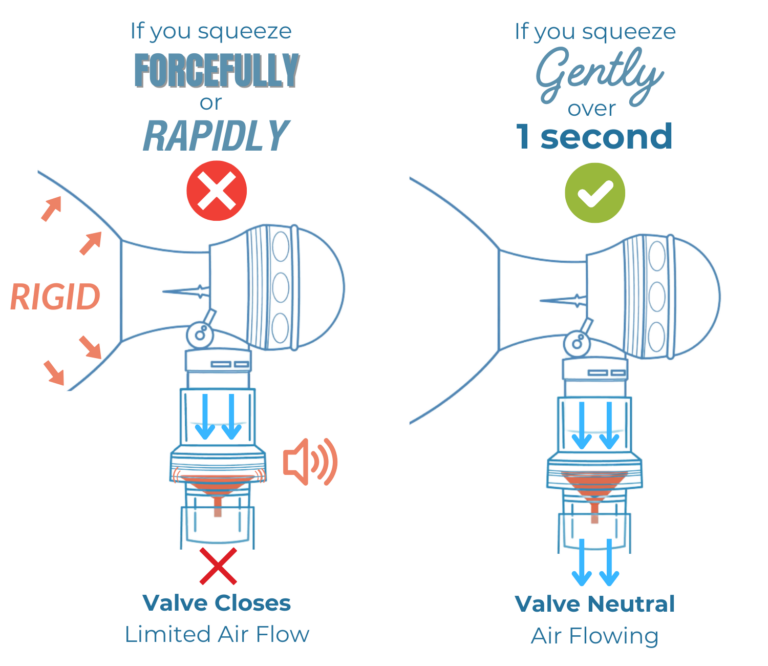
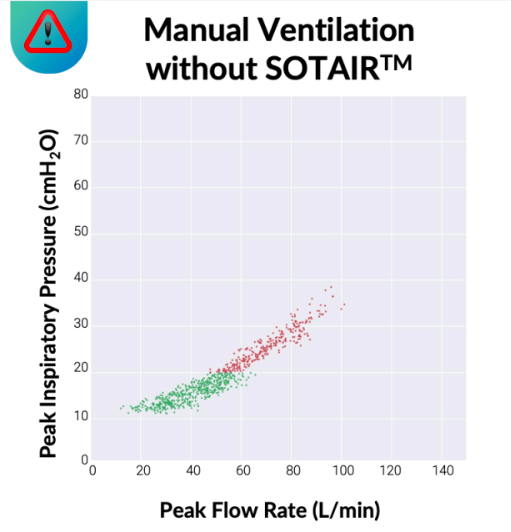
Sotair is a small, lightweight, easy-to-use flow control valve that fits between a manual resuscitator and a patient mask or airway. The valve prevents inspiratory flow rates from exceeding 55 LPM during manual ventilation, helping keep air delivery within safer limits without added cognitive load—no dials, screens, or additional equipment—allowing providers to stay focused on the patient.
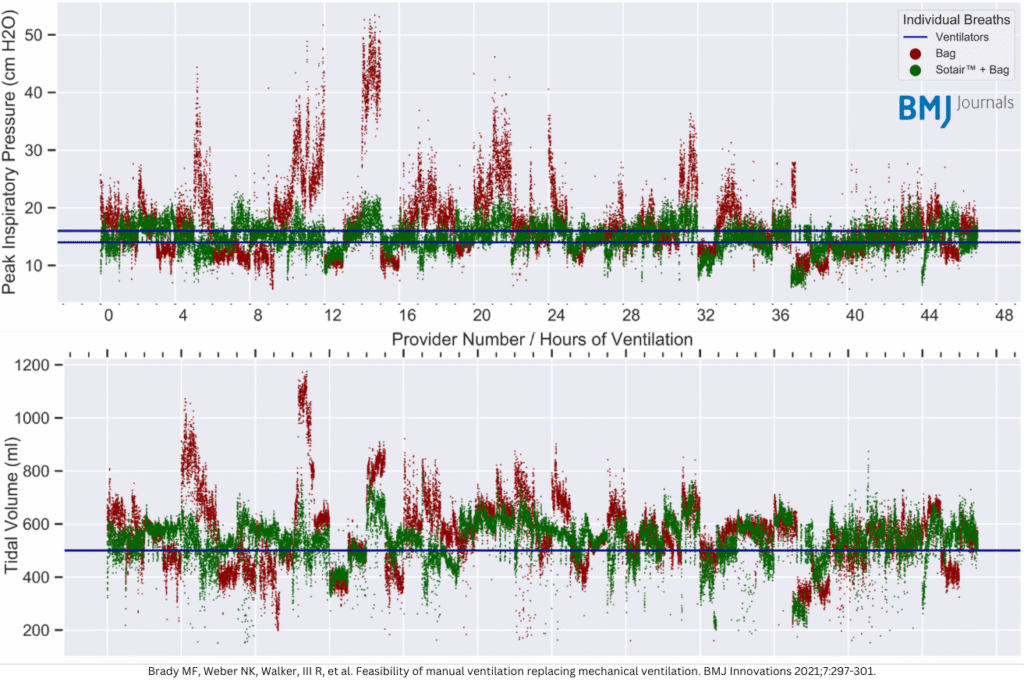
By regulating flow, Sotair helps reduce peak airway pressures, excessive tidal volumes, and excessive breath delivery rates, minimizing the risk of over-pressurization, over-ventilation, and hyperventilation.
Sotair’s user-friendly design requires approximately 30 seconds of training and provides multi-sensory feedback (haptic, auditory, and visual) to guide providers in real time—improving consistency and reducing variability during manual ventilation.